… the digital twin eliminates all idle times.
Time optimisation reduces demand to what is medically necessary.
The initial situation is ‘highly uneconomical’:
Hospitals treat large numbers of patients with small numbers of staff. Efficiency can theo-retically be realised with time planning and process control organised according to division of labour: important for expensive operating theatres – but – real operating times are not accidentally different from usual planning. Faulty planning formalism systematically ‘inflat-es’ operating theatre planning.
1st problem: The time deviations are considerable at ≈33%. As the calculation of person-nel requirements is based on ‘inflated’ OR scheduling, because it uses elements of collec-tively agreed working time, but the real time sequences follow medical activity times, arith-metical differences arise, especially as there is also no database of measured activity times. This creates widely distributed idle times in real processes, which results in ‘over-scheduling’ because unreal personnel requirements are added to the real ones.
2nd problem: Despite the inefficiencies, staff have become accustomed to their seemingly ‘unavoidable fate’. However, this can be changed – but not by improving conventional time organisation, but through digital time innovation.
Every status quo can and must be scrutinised!
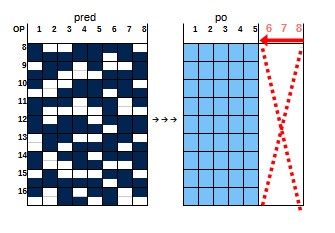
Time differences for individual operating theatre times (plan ≠ real)
Operating theatre scheduling is currently based on empirical values, estimates, average times and other subjective factors. There are no measured values or tests that prove the capability of this operating theatre scheduling. An audit would have to consist of two partial audits. A. The correspondence checks whether the operating theatre times derived from ‘empirical values’ correspond to the actual operating theatre times. B. Coding is used to ensure the identity of the number structures of the planned values and the number structures of the real OP times. The result determines the type of number (rational, fract-ional, natural numbers, etc.) and the associated arithmetic operations. Only after such a statistical check can the personnel requirements be calculated.
The subsequent examination shows that ‘experience values’ do not belong to any scale level. However, there is an unprofessional ‘substitute’: the largest medical activity time, the most atypical part of the real time dispersion, is ‘metrised to an empirical value’ and ‘ele-vated to a planned time’. Ordinal time becomes arithmetic time, so that the difficulty of scale irreversibility is miraculously ‘overcome’. At the same time, the much larger ‘exper-ience value’ is ‘superimposed’ on the majority of the much shorter real activity times as planned time. Planned times are created as ‘Coat times’, which contain a real part and an ‘inflated’ part. These numerous time buffers are the empty times of the 1st kind.
The operating theatre time processes are based on medical activity times. Their coding leads to ordinal scaling due to their medical character. The times also vary ordinally and are individual times due to the employee reference. Only their length can be measured. They are indivisible (an appendix is removed or not, but never half).
The status quo disappears on the basis of medical activity times
Time differences in the total volume of operating theatre time (plan ≠ real)
The current time planning uses the ‘planned times’ described above for the overall utili-sation of the operating theatre wing and supplements these with arbitrary time intervals between the operating theatre times. It is the division of labour among the full-time staff (FTE) that leads to idle times of the second kind. The reason for this is that individual full-time staff always have to deal with new individual specialities of the patients. Individual times cannot be planned. Consequence: The previous ‘experience value’ could also in-crease. If this were to occur, there would be an overlap between the surgeon’s own surgi-cal activity and the upstream and downstream surgical activity. To prevent this, empty tim-es of the second kind (buffers) are inserted between them. As an overlap could affect all full-time staff in the shift sequence, the empty times of the 1st and 2nd type are distributed across all operating theatres. Mathematically, highly inefficient NASH equilibria are formed that are difficult to change. They lead to ≈1/3 non-utilisation of the objectively usable total time capacity. During this time, the staff are medically inactive and can therefore be re-duced and utilised more economically elsewhere.
The uneconomical consequences of scheduling errors:
In the scheduling of knee TEP, the proportion of ‘planned time’ in the medical activity time is already very low (5.8%). In the overall OR planning, the proportion then proves to be statistically ineffective (1.6%). Inflated ‘Coat times’ cover up the real times. As the princip-le also applies to the other 16 planned operations, it leads to an overall overscheduling of ≈35% of the total time capacity.
During the period of overscheduling, full-time staff are formally regarded as busy and cannot be scheduled elsewhere during this time, even though they are not actually treating any patients. This has consequences in terms of time organisation. It leads to the creation of personnel capacities without medical activity. It leads to unreal personnel require-ments. This not only results in a loss of revenue, but is coupled with additional personnel costs: double inefficiency.
This status quo generates unreal personnel requirements
The solution: The digital twin
1. new time data:
- The individual time, both that of the operation as a whole and that of all sub-activities belonging to it, is measured for the individual full-time employee performing the operat-ion for each individual patient using sensors without any manipulation.
- It is checked for correspondence and coding. This ensures adequate statistical mapping of real times and enables the identity: Plan ≡ Real.
- A frequency table is created for each OR from individual times. It grows with each new execution. Its ordinal probability is permanently calculated.
- The probabilities show the confidence interval (>66%). The highest probability defines the planned operating theatre time.
2. new scheduling in the operating theatre wing:
- The ‘n’ registered operating theatres are sorted according to rank time.
- An event field ‚nn=x’ of possible operating theatre time sequences is generated from them. This set ‘x’ is broken down into ‘m’ operating theatres ‚m = Σmi’ disjoint time sub-sets. Ordinal time optimisation is used to search for the operating theatre time sequence that achieves a minimum time volume ‘nmi-min’ in each ‘mi’ among the ‘n’ scattered there. This is the OR sequence that scatters the least. Such OR time sequences exist in every ‘mi’. Their minimum ensures that all ‘mi’ scatter below the limit value of 5 min, i.e. are ‘quasiarithmetic’. Since: [nm1-min ≈ nm2-min ≈ … ≈ nmm-min] = n, the medical working times (ex-cluding idle time) are close to the collectively agreed working times below the significance threshold.
Consequence: These variables can therefore be used to plan both the full utilisation of the operating theatre wing and the volume of collectively agreed working hours. - This time planning for the operating theatre wing enables the content of the operating theatre wing to be planned in three dimensions (time, operating theatre, specialists).
3. new real time sequence in the operating theatre tract:
Positive and negative deviations are typical for scattering times. The real sequence is therefore permanently adapted to the schedule using ordinal PARETO time optimisat-ion.
The economic impact in relation to the original OR plan:
100% ≈ 54 ≈ 8 OP employees:
8 OP → 5 OP
Minimisation of personnel requirements: 54 → 34 = ─20 employees / day
Personnel cost savings: ≈ €1.300.000 / year
- The digital twin organises a smooth, fluid, time-dense process
- The rigid time scheme no longer applies
- All staff involved (surgeon, ward doctor, transport service,…) are informed of the end of the current operation and the start of the next one.
- The forecast function enables time estimation in the event of changes:
– Emergency, material failure, staff failure, operation cancellation,…)
– Fictitious, time-strategic queries: what if?
4. economic efficiency after minimising the personnel requirements in the example:
The software pays for itself. It ‘costs’ 70% of the savings on a one-off basis.
The economic effect: The internal rate of return: ro = 42.7%
You can calculate the actual personnel requirements for your own operating theatre processes.
Note: The intensive care unit and the differential diagnostic process are time-optimised in the same way as the operating theatre.